Ebola
What is the Ebola virus?
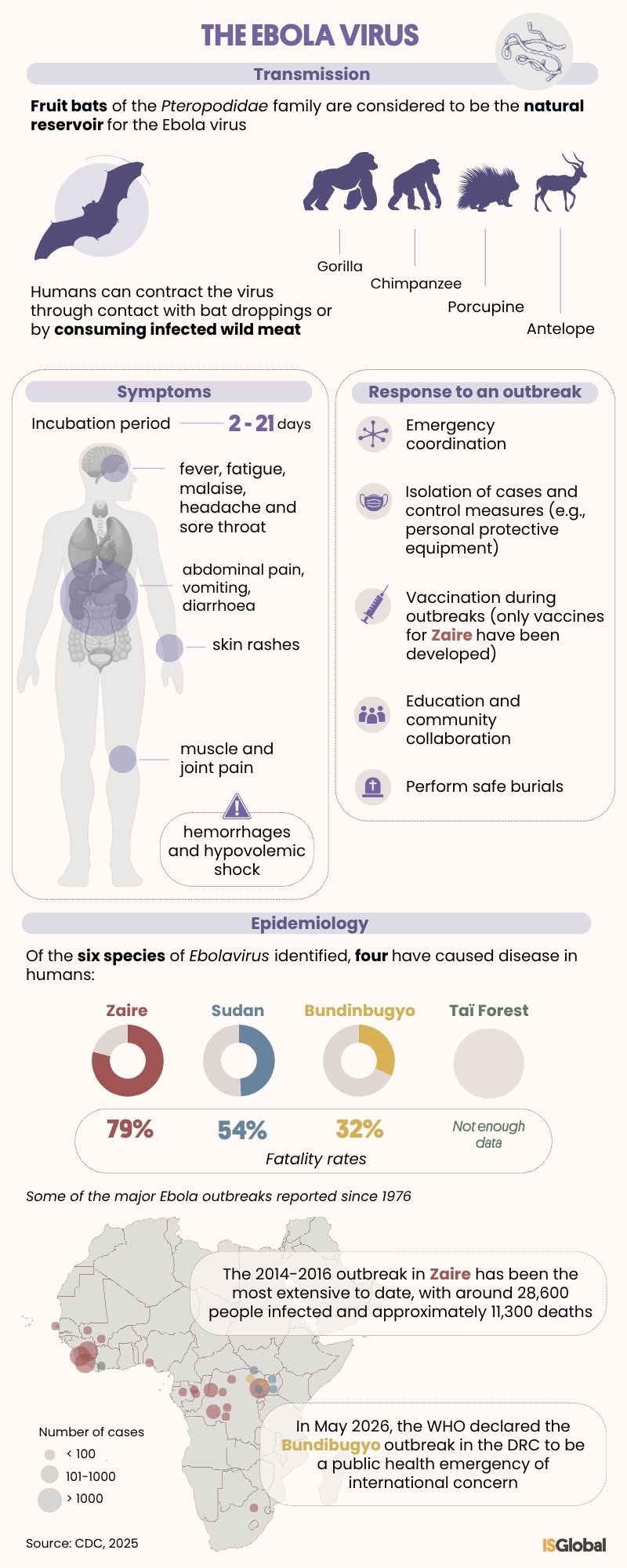
Ebola virus disease (EVD or Ebola) is an infectious disease caused by the Ebolavirus, a virus belonging to the Filoviridae family. Like Marburg fever, Lassa fever, hantavirus or dengue, Ebola can lead to viral haemorrhagic fever. These illnesses damage blood vessels and disrupt blood clotting, potentially causing haemorrhaging, organ failure and death. Ebola is classified as one of the so-called high-consequence infectious diseases (HCIDs), due to its high mortality rate, the lack of widely available treatments, the challenges involved in detecting it and its potential to spread within communities.
Of the six known species of Ebola virus, four can infect humans: Zaire (now referred to simply as “Ebola” by the WHO; it is responsible for the largest number of outbreaks and is also the deadliest), Sudan, Bundibugyo and Tai Forest. Mortality rates vary considerably depending on the strain: without treatment, the Zaire strain has an estimated fatality rate of around 79%, the Sudan strain around 54%, and the Bundibugyo strain approximately 32%.
Ebola is considered a zoonotic disease because its natural reservoir consists of fruit bats from the Pteropodidae family, found in subtropical regions of Africa, Asia and Oceania. The Ebola virus enters human populations through close contact with infected animals, even when the animals are dried out or mummified. Chimpanzees, gorillas, monkeys and other primates, as well as antelopes and porcupines, are also known to become infected with the virus.
Which Ebola outbreaks have been documented throughout history and what is the current situation?
Although the virus is believed to have existed for more than 10,000 years, it was first identified in 1976 during two simultaneous outbreaks in South Sudan and the Democratic Republic of the Congo (DRC), which resulted in 318 cases and 280 deaths. The outbreak in the DRC occurred near the Ebola River, from which the virus takes its name. Additional outbreaks were recorded in the following years, although they remained relatively limited in scale.
The 2014–2016 Ebola outbreak, caused by the “Zaire” species in West Africa, remains the largest and most complex outbreak to date: there were more cases and deaths than in all previous outbreaks combined, with around 28,600 infections and 11,300 deaths. It also spread across several countries, beginning in Guinea before reaching Sierra Leone and Liberia.
On 17 May 2026, the WHO declared the Ebola outbreak caused by the Bundibugyo species in the DRC and Uganda a Public Health Emergency of International Concern (PHEIC). According to the WHO, by 16 May there had already been 246 suspected cases, eight laboratory-confirmed cases and 80 suspected deaths reported in the Congolese province of Ituri, alongside several confirmed cases in Uganda.
The Bundibugyo species had previously caused outbreaks. The first was recorded in 2007 in the Bundibugyo district of Uganda, from which the species takes its name, resulting in 131 cases and 42 deaths. In 2012, another outbreak in Isiro, then part of the DRC’s Orientale Province, affected 57 people and caused 29 deaths.
Transmission of the Ebola virus
The virus is transmitted to humans through contact with bat droppings or the consumption of infected bushmeat. It is then spread from person to person through close and direct physical contact, but it is not airborne.
Transmission occurs through direct contact with the bodily fluids of infected individuals or corpses, particularly blood, vomit, faeces and other bodily fluids. Less commonly, sexual transmission may also occur, as the virus can remain temporarily in certain tissues even after clinical recovery.
The Ebola virus may also spread through contact with contaminated surfaces and objects, although the risk is lower, especially when proper disinfection procedures are followed.
Symptoms
The incubation period of the Ebola virus — the time between infection and the onset of symptoms — ranges from two to 21 days. Initial symptoms are non-specific and include fever, fatigue, general malaise, headache, sore throat, abdominal pain, and muscle or joint pain. As the disease progresses, patients may develop vomiting, diarrhoea, skin rashes and signs of impaired liver and kidney function.
Haemorrhaging may occur in the later stages of the illness. This can involve internal or external bleeding, including blood in vomit or stools, as well as nosebleeds, bleeding gums or vaginal bleeding. When the central nervous system is affected, symptoms such as confusion, irritability or aggressive behaviour may appear. Death may result from haemorrhage and hypovolaemic shock, which occurs when the body loses a significant amount of blood.
Diagnosis
Diagnosing Ebola can be challenging during the early stages of the disease, as its initial symptoms resemble those of other common infections such as malaria or typhoid fever.
Definitive confirmation relies on specialised laboratory tests capable of detecting the virus’s genetic material, its antigens, or the antibodies produced by the body in response to infection. Commonly used techniques include RT-PCR testing, ELISA assays and viral isolation in cell cultures. Because handling patient samples involves a high biological risk, these analyses must be carried out in maximum-security laboratories under strict biosafety protocols and with specialised sample transport procedures.
Treatment of Ebola
Treatment for Ebola focuses on supporting the patient’s vital functions in order to improve survival chances. This includes intravenous fluid replacement, monitoring blood pressure and oxygen levels, pain relief and nutritional support. Early medical intervention is crucial, as it significantly improves clinical outcomes.
In recent years, targeted therapies based on monoclonal antibodies have been developed, including mAb114 (Ansuvimab™) and REGN-EB3 (Inmazeb™), which are effective against the Ebola virus formerly known as “Zaire”. However, there are still no approved treatments for other variants such as the Sudan or Bundibugyo viruses, although clinical trials and the development of new drugs and vaccines are ongoing. Experimental therapies have also been explored, including plasma transfusions from survivors and antivirals such as favipiravir, brincidofovir and TKM.
Vaccines
Several vaccines targeting the Zaire species have been approved. Among the most important are rVSV-ZEBOV (Ervebo, Merck, 2019), primarily used for rapid outbreak response, and the Zabdeno/Mvabea combination (Janssen, 2020), which follows a two-dose schedule administered several weeks apart and is designed to provide longer-lasting protection between outbreaks. Both vaccines are used to protect healthcare workers and others at high risk of exposure. Research is continuing into vaccines for other Ebolavirus species, including Sudan and Bundibugyo.
How can Ebola be prevented?
Key prevention measures include rapid coordination of the public health response, early diagnosis, contact tracing, case isolation, vaccination during outbreaks, and strict hygiene and infection-control measures in healthcare settings. Community engagement is essential to support early detection, encourage acceptance of public health measures and ensure safe burial practices, as some funeral rituals may facilitate transmission of the virus.
Health education and risk communication also play a vital role in reducing exposure to potentially infected animals and contact with the bodily fluids of infected individuals.
READ MORE
COLLAPSE
- Treating Every Outbreak as Though It Were Occurring in Our Backyard(ISGlobal, 2026)
- From Curiosity to the Fight Against Deadly Viruses: My Journey with Ebola and Nipah(ISGlobal, 2026)
- ISGlobal’s Response over the Course of the Ebola Epidemic(ISGlobal, 2016)
- Ebola. A Bitter Celebration(ISGlobal, 2016)
- A Maternity Ward during the Ebola Outbreak: My Experience as an Ebola Fighter(ISGlobal, 2015)
- Spain is Not Free of Ebola(ISGlobal, 2014)
- Taking a leap of faith in the fight against Ebola(ISGlobal, 2014)
- Ebola virus: From obscurity to a threat(ISGlobal, 2014)