Steatotic Liver Disease

What is Steatotic Liver Disease?
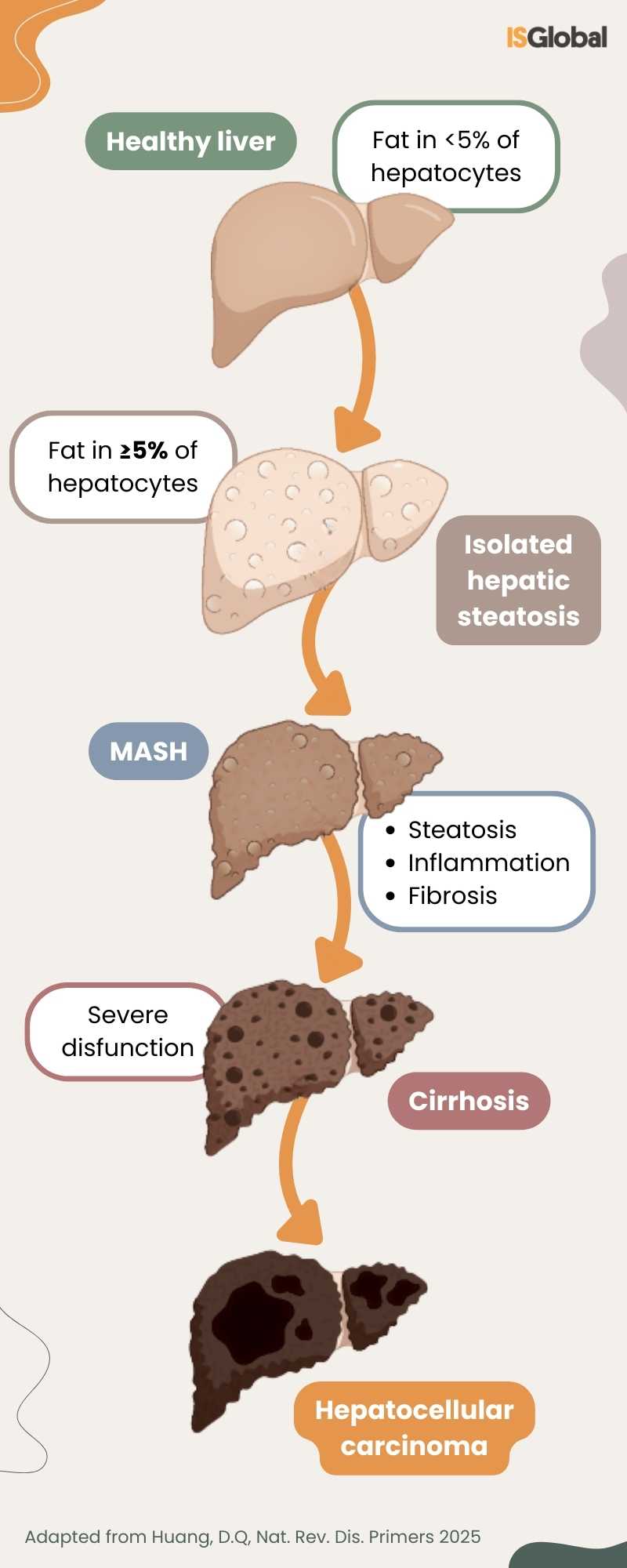
Steatotic liver disease (SLD), formerly known as “fatty liver disease”, covers a range of conditions in which fat accumulates within hepatocytes, the cells that make up the majority of the liver.
This accumulation is not always accompanied by liver damage, as the liver is an organ with high metabolic and detoxifying capacities. However, excess fat in the liver is unhealthy, and when it is stored in excess — that is, when more than five percent of liver tissue contains fat — the organ responds with inflammatory mechanisms.
The Broad Spectrum of SLD
SLD includes various diseases; in all of them, fat accumulates in the liver, but they have different causes and clinical courses.
When metabolic factors predominate, such as obesity, insulin resistance, type 2 diabetes, or cardiovascular disease, the condition is called metabolic dysfunction-associated steatotic liver disease (MASLD). It is not associated with alcohol consumption and is estimated to affect at least 30% of the adult population.
When alcohol consumption is the primary cause of steatosis, the term alcohol-related liver disease (ALD) is used, and when both factors — metabolic and alcoholic — interact significantly, it is referred to as metabolic dysfunction and alcohol-related liver disease (MetALD).
Over time, fat accumulation in the liver can progress to a more severe inflammatory form, known as metabolic dysfunction-associated steatohepatitis (MASH). When this occurs, liver cells begin to be damaged, increasing the risk of developing fibrosis (scarring of liver tissue). If the scar tissue replaces healthy liver tissue and impairs its function, it is called cirrhosis. In advanced stages, the risk of developing liver cancer also increases.
Its Impact on Public Health
Steatotic liver disease is considered a threat to public health, not only due to its potential to progress to diseases such as cirrhosis or liver cancer (particularly hepatocellular carcinoma, the most common type), but also because of its association with cardiovascular and metabolic disorders, which increase related complications and morbidity and mortality.
Globally, chronic liver disease is responsible for nearly 2 million deaths per year (including hepatitis B and C infections), with a significant proportion attributable to liver cancer.
Equity in the management of steatotic liver disease
Ensuring an equitable approach to liver disease requires recognising that certain groups have additional vulnerabilities.
One example is people living with HIV. They represent a population at particularly high risk due to several factors, including chronic immune activation induced by the infection, a higher prevalence of metabolic comorbidities — such as diabetes and dyslipidaemia — and accelerated ageing, which is observed more frequently in this population. Additionally, some antiretrovirals may alter liver metabolism and, in certain cases, promote fat accumulation in the liver.
Diagnosis of Steatotic Liver Disease
The diagnosis of SLD combines clinical assessment with analytical and imaging tests, which allow the detection of fat presence and the risk of liver fibrosis without the need for invasive procedures. When confirmation of inflammation and fibrosis is required, liver biopsy remains the reference standard but is usually unnecessary, reserved for cases with diagnostic uncertainty or where certainty regarding the degree of liver damage is required.
Treatment of Steatotic Liver Disease
The cornerstone of treatment is the modification of risk factors that promote fat accumulation in the liver. The goal is to reduce metabolic stress on this organ, improve insulin sensitivity, and halt inflammation.
Diets based on fresh foods, rich in fibre and healthy fats, such as the Mediterranean diet, are recommended. At the same time, ultra-processed foods should be avoided, as they promote fat accumulation in the liver and worsen metabolic health.
When alcohol is a significant factor in the disease (as in ALD or MetALD), the recommendation is clear: reduce it significantly or ideally eliminate it completely. Patients with metabolic SLD with scarring (significant fibrosis) may also benefit from alcohol abstinence.
Physical activity is another essential pillar. Both aerobic exercise and resistance training help reduce liver fat, even without evident weight loss.
Pharmacological treatment for steatotic liver disease is advancing: in the USA, two drugs for MASH are already approved, resmetirom (Rezdiffra) and semaglutide (Wegovy). However, in the European Union, only resmetirom (Rezdiffra) has currently received authorisation for treating MASH with fibrosis. These options complement lifestyle interventions, which remain the foundation of treatment.
The importance of preventive hepatology and integrated care
Preventive hepatology aims to reduce the burden of liver disease within the population by acting before the condition progresses to inflammatory or irreversible stages. In this way, it focuses on identifying risk factors and modifying them.
Early detection and lifestyle interventions not only prevent the progression of liver damage but can also reverse steatosis in many cases.
Optimal, multidisciplinary management of SLD benefits from an integrated care approach, in which hepatology specialists, GPs and primary care nurses, nutritionists, mental health professionals and physical activity specialists work together to address all determinants of the disease. This facilitates early detection of complications and strengthens patients’ adherence to medical recommendations.
READ MORE
COLLAPSE
- Steatotic Liver Disease, a Public Health Threat in Barcelona(ISGlobal, 2025)
- Breaking it Down: Eliminating the Impact of Viral Hepatitis Starts with Recognizing Liver Health as a Global Priority(ISGlobal, 2025)
- Living With Diabetes. Working For Change(ISGlobal, 2025)
- The Silent Impact of Liver Diseases(ISGlobal, 2024)
- First-Ever Side-Event on Under-Recognised Liver Diseases Held During United Nations General Assembly Week(ISGlobal, 2024)
- World Experts Set a Global Agenda to Tackle the Growing Burden of Steatotic Liver Disease(ISGlobal, 2023)
- Comprehensive Models of Care for Non-Alcoholic Fatty Liver Disease (NAFLD)(ISGlobal, 2021)
MULTIMEDIA MATERIAL